
2027 Medicare Advantage and Part D Rate Announcement
A More Stable Stable Base for Evidence-based Risk Adjustment is Here
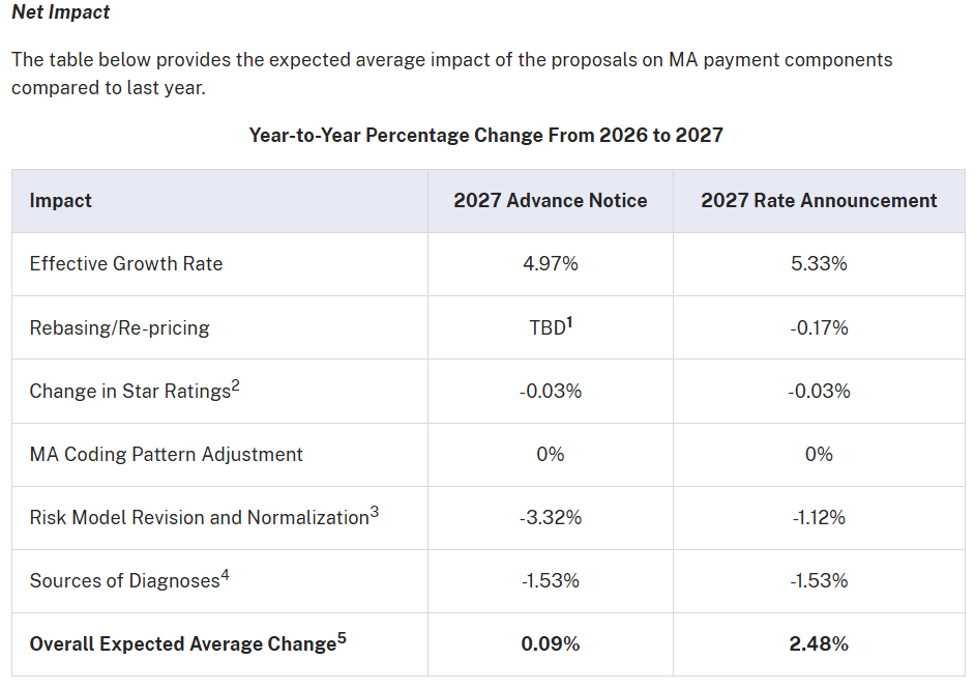
CMS has released the final CY 2027 Medicare Advantage and Part D Rate Announcement, and the overall message for health plans and provider organizations is reassuring: the final policy is more favorable and more stable than initially proposed, while continuing to guide the industry toward stronger, evidence-based risk adjustment practices.
Compared to the Advance Notice, CMS has taken a more measured approach…resulting in an expected 2.48% increase in MA payments. This creates a more predictable financial environment for 2027 planning.
Reference – https://www.cms.gov/newsroom/fact-sheets/2027-medicare-advantage-part-d-rate-announcement
One of the most impactful updates in the final announcement is CMS’s decision to maintain the current Part C risk adjustment model (2024 model) for CY 2027.
This is a meaningful departure from the Advance Notice, where CMS had proposed introducing a newly recalibrated model using more recent data. By not moving forward with that change, CMS has provided:
- Continuity in RAF calculations
- Reduced volatility in financial forecasting
- More time for organizations to adapt to recent model transitions
Continued Focus on Diagnosis Validity and Data Integrity
While CMS paused on model changes, it did finalize key policy updates that emphasize the importance of how diagnoses are captured and supported.
- Exclusion of Audio-Only Diagnoses
Diagnoses captured through audio-only encounters will no longer be eligible for risk adjustment.
While CMS estimates minimal aggregate financial impact, the operational implications are important:
- Greater emphasis on in-person or video-supported care
- Stronger alignment between clinical interaction and diagnosis capture
- Reduced reliance on less substantiated documentation pathways
Proven Strategic Value
CMS also finalized the exclusion of unlinked chart review diagnoses—those not tied to a specific patient encounter.
An exception remains for members switching plans, which helps reduce disruption during transitions. However, the broader direction is clear:
- Diagnoses must be traceable to encounters
- Standalone chart abstraction is becoming less impactful
- Clinical and coding workflows must be more tightly integrated
This policy signals a continued move toward greater auditability and program integrity. Key Operational and Compliance Challenges Under New CMS Guidelines
# | Problem Area | Description | Impact |
1 | Compliance Risk from Unlinked Diagnoses | Diagnoses are not consistently tied to valid patient encounters | Increased CMS audit risk and potential revenue loss |
2 | Declining ROI from Retrospective Reviews | Over-reliance on chart abstraction with decreasing effectiveness under new CMS rules | Wasted effort on low-value reviews and reduced financial return |
3 | Disconnected Clinical & Coding Workflows | Coding activities are not integrated into provider or EMR workflows | Missed opportunities to capture conditions during visits |
4 | Limited Audit Readiness & Traceability | Lack of clear linkage between diagnosis, clinical evidence, and encounter | Higher compliance risk and difficulty defending audits |
5 | Fragmented Data & Operational Inefficiency | Disparate systems (claims, EMR, coding) and inefficient chart chase processes | Poor prioritization, low productivity, and limited visibility |
Normalization Remains—But Execution Now Matters More
Normalization continues to act as a moderating factor on RAF growth, but the final impact is significantly less severe than initially proposed.
- Advance Notice estimate: -3.32% impact
- Final estimate: -1.12% impact
This change provides meaningful relief for plans, allowing coding improvements to translate more effectively into financial outcomes.
Part D Updates – More focus needed by MA PD Plans
Unlike Part C, CMS did finalize updates to the Part D risk adjustment model, incorporating:
- More recent data (2023 diagnoses, 2024 costs)
- Similar exclusions for audio-only and unlinked chart review diagnoses
These updates are designed to improve predictive accuracy and alignment with evolving benefit structures, making pharmacy-related risk adjustment an increasingly important strategic focus.
What Does This Mean for Organizations:
The final CY 2027 announcement strikes a balance between financial stability and continued policy evolution. For health plans and provider organizations.
- CMS is driving a shift toward encounter-based, evidence-driven risk adjustment, reducing reliance on retrospective and unsupported capture methods.
- Unlinked chart reviews and audio-only diagnoses will no longer drive value—creating risk of missed RAF despite identified conditions.
- Organizations must move to Evidence-Driven Recommendation (EDR)-driven workflows, converting insights into provider actions and encounter-based documentation.
- IHA and telehealth vendors need to prioritize audio-video visits or ensure rapid follow-ups, with strong tracking of conversion to valid encounters.
- Chart review programs should evolve into provider-integrated, real-time, encounter-linked models.
- Part D risk adjustment now requires dedicated prioritization, with stronger integration of pharmacy data and clinical validation.
The Bottom Line
The final CY 2027 Rate Announcement provides a more favorable and predictable financial outlook than initially expected. At the same time, it reinforces a long-term transition toward greater accountability, transparency, and clinical validity in risk adjustment. Winning organizations will align analytics, provider workflows, and data integrity to ensure every identified condition is captured compliantly.


